Signs and symptoms of spinal muscular atrophy (SMA)
SMA symptoms may include progressive muscle weakness, floppiness, and muscle wasting (atrophy). Muscle weakness is usually the same on both sides of the body
Individuals with SMA may experience symptoms differently, and the disease is divided into types based on age of onset and highest motor milestone achieved. There is also a range of severity within each type, and as many as 25% of individuals may not have a precise type.
Progressive weakness of muscles used to chew and swallow
Poor muscle tone
“Frog-leg” posture when lying
Severe muscle weakness on both sides of body
Progressive weakness of muscles that help in breathing (intercostal muscles)
Highest motor milestone achieved
ABLE TO SIT INDEPENDENTLY
(“sitters”)
Life expectancy
>2 YEARS
70% STILL LIVING AT AGE 25
Type
II (also known as Dubowitz disease)
Characteristics
Muscle weakness
Swallowing, coughing, and breathing problems may occur but are typically less common
Muscle aching and joint stiffness symptoms
Children may develop spinal problems such as scoliosis (curvature of the spine), which may require bracing or surgery
Highest motor milestone achieved
ABLE TO WALK
INDEPENDENTLY
(“walkers,” although they may progressively lose this ability)
Life expectancy
NORMAL
Type
III (also known as Kugelberg-Welander disease)
Characteristics
Scoliosis
Swallowing difficulty
Muscles in the legs are generally more severely affected than the arms
Muscle aching
Joint overuse symptoms
Highest motor milestone achieved
ALL
Life expectancy
NORMAL
Type
IV
Characteristics
Physical symptoms are similar to juvenile-onset spinal muscular atrophy, with the gradual onset of weakness, tremors, and muscle twitching first noted in late teens or early adulthood
There are other diseases that are similar to spinal muscular atrophy, but have different genetic causes. These conditions include:
Spinal muscular atrophy with respiratory distress (SMARD)—SMARD has similar symptoms to infant-onset spinal muscular atrophy, though it affects the upper spinal cord neurons instead of the lower motor neurons. Children with SMARD typically have low birth weight and experience symptoms within the first 3-6 months, including severe respiratory distress due to paralysis of the diaphragm
Distal hereditary motor neuropathy (sometimes referred to as Type V SMA)—Distal hereditary motor neuropathy is an extremely rare autosomal dominant genetic disease, which means that only 1 inherited copy of the abnormal gene is required for the disease to occur. Distal hereditary motor neuropathy affects nerve cells in the spinal cord and presents as weakness and wasting that starts in muscles of the upper and lower limbs and spreads later to other muscles
Kennedy’s disease (KD)—Unlike spinal muscular atrophy, which affects the motor neurons, KD affects both lower motor and sensory neurons and only occurs in males. KD is a disease of the X chromosome, occurring in approximately 1 in 40,000 males
For more information about spinal muscular atrophy, visit Cure SMA. To learn more about other rare diseases, please visit the following websites:
For children with spinal muscular atrophy, the disease is often first suspected by a parent, who may notice that their child is not meeting certain developmental milestones
Parents may observe that their child is not reaching typical physical milestones for their age, such as the ability to hold their head up, to roll over, or to sit up independently. Swallowing or feeding may also become difficult, and children may lose the ability to swallow safely without choking or inhaling food into the lungs (aspiration).
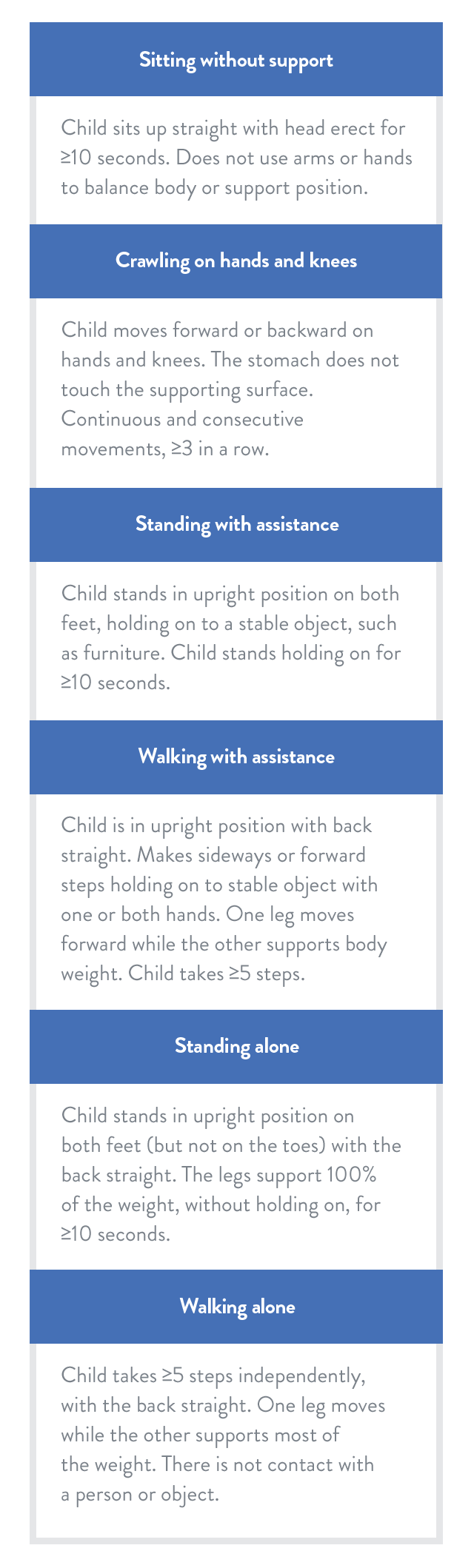
While all babies develop at their own pace, the World Health Organization (WHO) offers the following general motor milestone guidelines as part of the Multicentre Growth Reference Study (MGRS):
Motor milestones in the MGRS
Adapted from the WHO Multicentre Growth Reference Study.
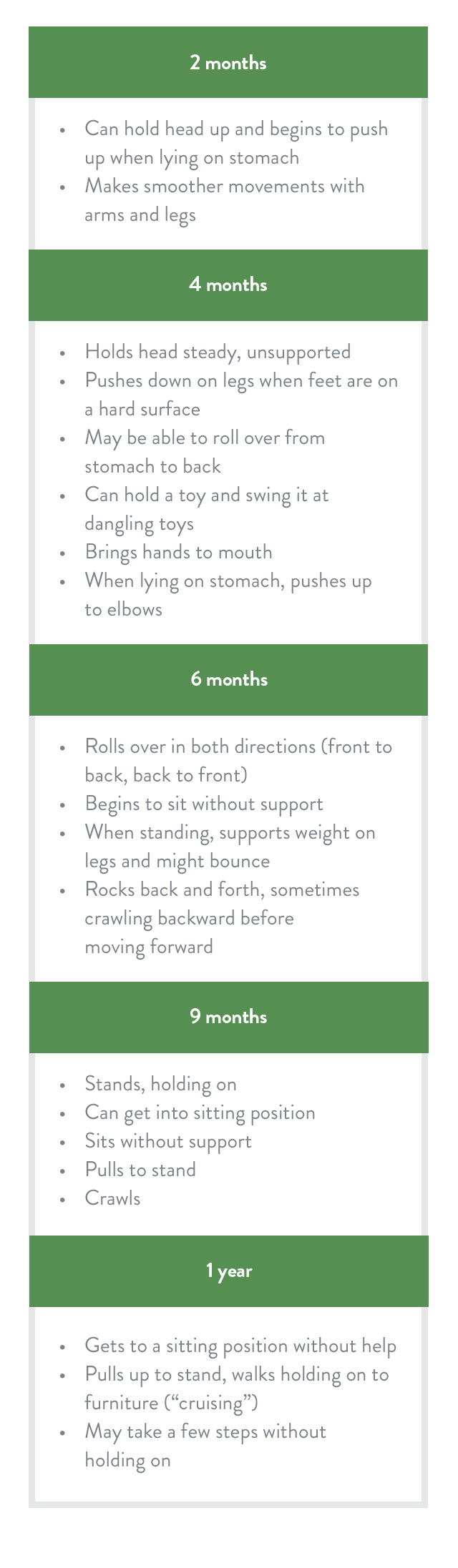
Adapted from the Centers for Disease Control and Prevention Milestone Checklist.
Parents’ reports of their children’s gross motor development tend to be reliable. Sharing observations of potential motor delays with a doctor can help to determine an appropriate SMA care strategy.